Blog
The History of Evolving Technology (Glasses, RK & LASIK)
The History of Evolving Technology of Vision Correction, Part 1
Refractive error (blurry vision due to an imbalance between the length of the eye and the curvature of the cornea/lens in the front of the eye) comes in four forms, as described earlier: myopia (nearsightedness), hyperopia (farsightedness), stigmatism (or toricity, meaning different corneal curvatures), and presbyopia (age-related loss of zooming power of the eye).
Refractive surgery has been one of the most popular methods in the past.
Surgery to correct these conditions is known as refractive surgery. Many techniques have been used in the past, and many new techniques are currently being used. The most common problem we treat is myopia, which affects about 40% of the U.S. population. Recently, an article was published in a scientific journal about the myopia “epidemic” in the United States. Since the 1970s, myopia has increased from 25% of the population to over 40%, likely due to the effect of computers and hand-held devices on the development of the eye. These conditions have been treated with glasses for the last few hundred years, and with contact lenses since the 1940s.
The first Internal Radial Keratotomy was performed in 1940.
In Japan, Dr. Tsutomu Sato first performed “Internal Radial Keratotomy (RK)” for nearsighted patients in the 1940s by using a knife to make slits within the cornea in order to weaken and flatten it. This initially worked well, but most patients ended up needing a corneal transplant due to damage to cells on the inside of the cornea that keep it clear. In Russia in the 1970s, Dr. Svyatoslav Fyodorov popularized RK performed on the outside of the cornea. He is well known for performing this surgery with colleagues on a rotating operating table with each surgeon performing a different task.
Learn more about LASIK and if it’s the right fit for you.
Unfortunately, RK isn’t always the final solution to vision problems.
RK surgery worked well for mild nearsightedness, and was brought to the United States in the early 1980s. Hundreds of thousands of procedures were performed with good results. The problem with RK was that the higher the prescription, the poorer the accuracy of the procedure. Also, after about a decade of tracking patients, it became evident that about 40-50% of those having the procedure would not have a stable result and become farsighted instead of nearsighted, requiring glasses or contacts again. Many of these patients are now requiring laser or lens surgery in order to see better without glasses.
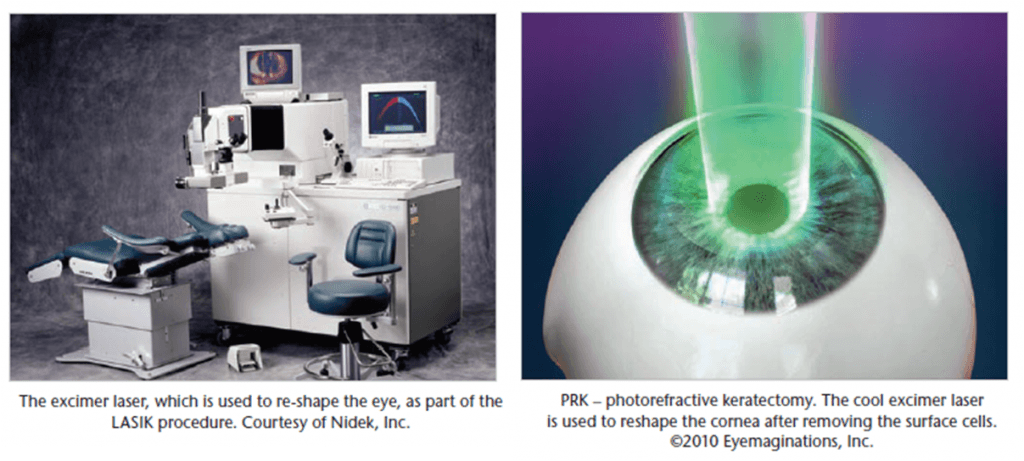
As an alternative to RK, the excimer laser was developed in the late 1980s to treat refractive error by the cool sculpting of the corneal tissue, rather than making cuts to weaken the cornea. In 1987, this laser was first used on the surface of the human cornea after removing the surface cells in a procedure called PRK (photorefractive keratectomy). PRK was more accurate
and stable then RK, but was somewhat uncomfortable and associated with blurry vision for a few weeks afterward while the surface cells re-grew over the eye. PRK (flapless LASIK) is still used today for patients who cannot have LASIK because of thin or abnormally shaped corneas. The FDA approved PRK for use in the United States in 1995.